Proximale humerusfractuur
Proximale humerusfractuur
Auteur: J. Sprakel, MD - Laatste update: 19-02-2017
Proximale humerusfractuur

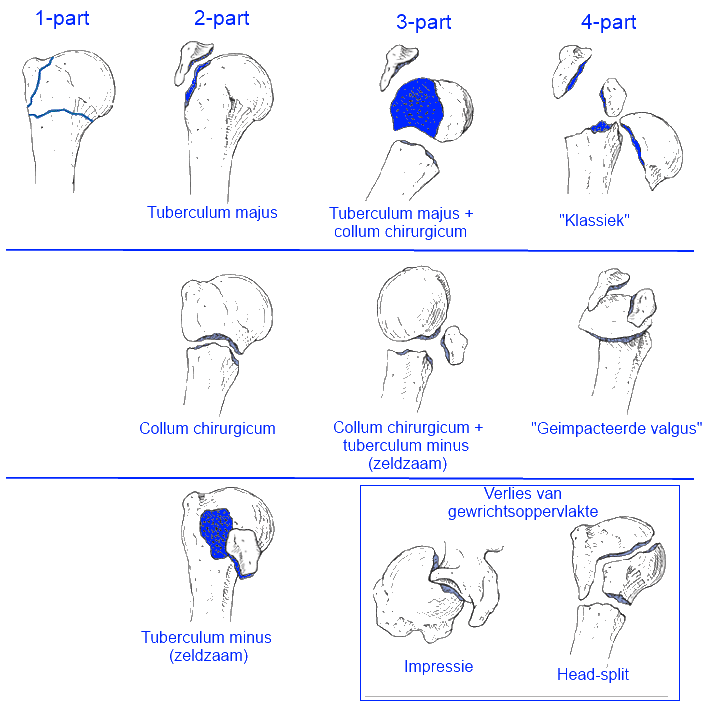
Classificatie
- - Neer-classificatie: De criteria voor dislocatie is 45 graden angulatie of meer dan 1 cm dislocatie tussen fractuurdelen. Indien dislocatie minder is, dan wordt er gesproken van minimale dislocatie, ondanks het aantal fracturen.
- - 1-part: Niet gedisloceerde fracturen
- - 2-part: Fractuur collum chirurgicum of tuberculum majus of tuberculum minus met dislocatie
- - 3-part: Fractuur collum chirurgicum met tuberculum majus of tuberculum minus met dislocatie
- - 4-part: Fractuur collum chirurgicum, tuberculum makus, minus en collum anatomicum
Conservatieve behandeling
-
Indicaties
- - Alle 1-part fracturen
- - Stabiele 2 & 3 part fracturen met geringe dislocatie
- - Geïmpacteerde fracturen
- - Kinderen
- - Gedisloceerde fracturen indien
- * ernstige osteoporose
- * significante co-morbiditeit
- * lage compliance
- - Functioneel
- - Immobilisatie met collar en cuff gedurende 2 a 3 weken
- - 1ste week rust
- - 2de & 3de week slingeroefeningen (op geleide van klachten uitbreiden)
- - Controle na 1 week met uitleg + X-controle schouder AP & Y (cave: secundaire dislocatie)+ oefeninstructies meegeven, fysiotherapie op indicatie
- - Controle na 3 weken
- - Controle na 6 weken
- Fase 1 (3 weken): Immobilisatie
- - Immobilisatie voor 2 weken
- - Slingeroefeningen
- - Voorzichtig geassisteerde bewegingen
- - Vermijden externe rotatie in de eerste 6 weken
- Fase 2 (week 3-9): Passieve/geassisteerde range of motion
- - Actief geassisteerde anteflexie en abductie oefeningen
- - Voorzichtig functioneel gebruik in week 3 t/m 6 (geen abductie tegen weerstand)
- - Geleidelijk afbouwen van geasssisteerde oefeningen vanaf week 6
- Fase 3 (week 9): Progressieve weerstandoefeningen
- - Isotone, concentrische en eccentrische weerstandsoefeningen
- - Indien gewrichtstijffheid met botgenezing dan starten met passieve strekoefeningen door fysiotherapeut
(Na-)behandeling
Follow-up:
Fysiotherapeutisch behandelschema
Functiecontrole:
 |
 |
 |
||
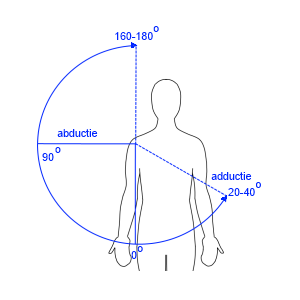
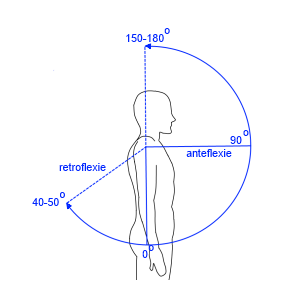
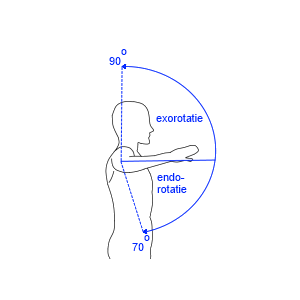
| Abductie / Adductie | Anteflexie / Retroflexie | Endo- / exorotatie bij arm naast lichaam met 90° gebogen elleboog met palm omhoog | Anteversie / retroversie bij arm loodrecht in transversale vlak | Endo- / exorotatie bij arm in 90° abductie met 90° gebogen elleboog |
| 180° - 0° - 40° | 180° – 0° – 50° | 70° – 0° – 60° | 160° – 0 °– 50° | 70° – 0° – 90° |
Operatieve behandeling
-
Indicaties
-
1-part fractuur van tuberculum majus:
- >3mm dislocatie (sportatleten)
- >5 mm dislocatie (jong actieve mensen)
- >10mm dislocatie (ouderen)
- - 2-3 part fracturen met ongunstige prognostische factoren:
- Medial hinge >1cm
- Varus
- Dislocatie > 1/2 schachtbreedte humerus
- Verplaatsing tuberculum majus in subacromiale ruimte - - 4-part fracturen en intra-articulaire luxatie fracturen
- Headsplit
- Impressie - Philos-plaat of Multiloc proximal humeral nail
- Arthroplastiek
- - Head split fracturen, zonder perfusie van de humeruskop
- - Niet reconstruceerbare fracturen jonge patienten (hemiarthroplastiek)
- - Ouderen met complexe 3-4 part met slechte botkwaliteit (reversed arthroplastiek)
- - Controle na 2 weken met uitleg + hechtingen verwijderen + oefeninstructies meegeven + start fysiotherapie
- - Controle na 6 weken + functiecontrole + X-controle schouder AP & Y
- - Controle na 12 weken + functiecontrole + X-controle schouder AP & Y
(Na-)behandeling
Follow-up:
Functiecontrole:
|
|
|
||
| Abductie / Adductie | Anteflexie / Retroflexie | Endo- / exorotatie bij arm naast lichaam met 90° gebogen elleboog met palm omhoog | Anteversie / retroversie bij arm loodrecht in transversale vlak | Endo- / exorotatie bij arm in 90° abductie met 90° gebogen elleboog |
| 180° - 0° - 40° | 180° – 0° – 50° | 70° – 0° – 60° | 160° – 0 °– 50° | 70° – 0° – 90° |
Complicaties
- Conservatieve behandeling: 1
- - Functiebeperking, voornamelijk bij extensie, gemiddeld 30o
- - Avasculaire necrose (0,8%)
- - Secundaire dislocati of instabiliteit (0,8%)
- - Symptomatische malunion (4%)
- - Non-union (4%)
- - Frozen shoulder (4%)
- - Rotator cuff letsel (0,8%)
- - CRPS
- Operatieve behandeling: 1
- - Functiebeperking ondanks geslaagde osteosynthese
- - Wondinfectie (1,6%)
- - Zenuwletsel (1,6%)
- - Avasculaire necrose (3,2%)
- - Secundaire dislocatie of instabiliteit
- - Osteosynthese materiaal problemen / migratie (8%)
- - Symptomatische malunion (3,2%)
- - Non-union
- - Frozen shoulder (4,8%)
- - Rotator cuff letsel (2,4%)
- - Re-operatie (9%)
- - CRPS (0,8%)
- - Pneumothorax


Referenties
- 1. Rangan A, Handoll H, Brealey S, Jefferson L, Keding A, Martin BC, Goodchild L, Chuang LH, Hewitt C, Torgerson D; PROFHER Trial Collaborators. Surgical vs nonsurgical treatment of adults with displaced fractures of the proximal humerus: the PROFHER randomized clinical trial. JAMA. 2015 Mar 10;313(10):1037-47.