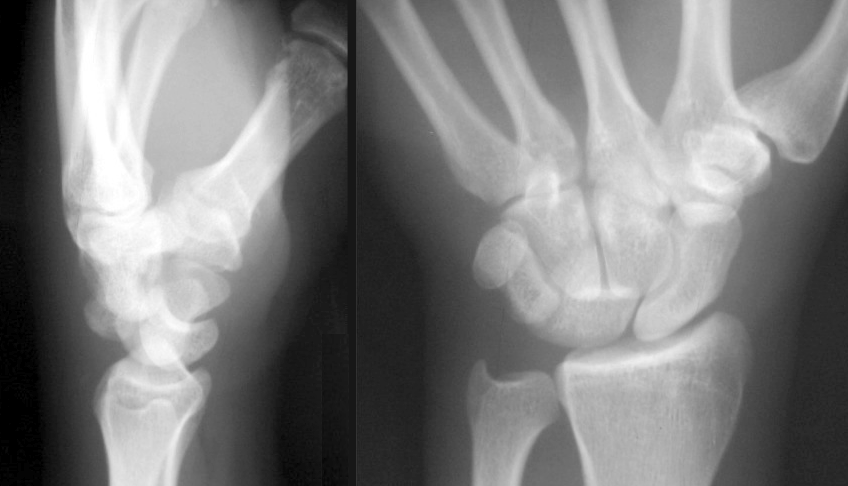
Perilunaire luxatie
Perilunaire luxatie
Auteur: J. Sprakel, MD - Laatste update: 08-10-2017
Perilunaire luxatie

Classificatie
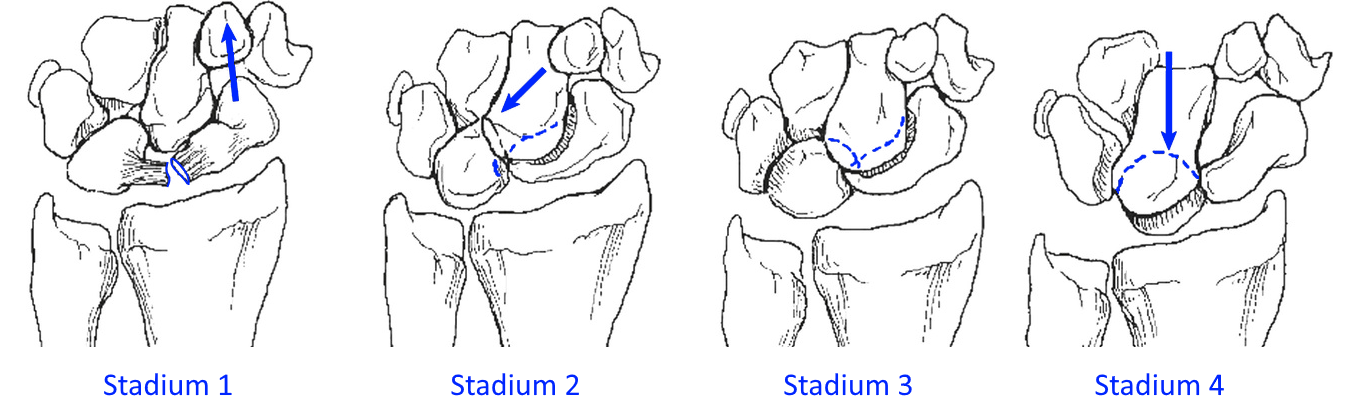
- Classificatie volgens Mayfield 6
- Stage 1: Scaphoidfractuur of SL-dissociatie of beide
- Stage 2: Dislocatie van capitatum en gehele carpalia naar dorsaal
- Stage 3: TL-diastase en rotatie triquetrrum, volaire triquetrumfractuur
- Stage 4: Dislocatie van lunatum naar volair, met carpus in lijn met radius
- Subdivisie 7
- Lesser arc letsel: Alleen ligamentair letsel:
- - Ruptuur van scapholunaire ligament gevolgd door lunatocapitate dislocatie en lunotriquetrale disruptie
- Greater arc letsel: in combinatie met fractuur:
- - Os scaphoideum
- - Os capitatum
- - Os lunatum
- - Os triquetrum
- - Os hamatum
- - Processus styloideus radii
Classificatie volgens Mayfield 6
Operatieve behandeling
- Indicaties:
- - Allle perilunaire luxaties
- (Na-)behandeling:
- - Initieel repositie om druk van n. medianus, weke delen en kraakbeen te verlagen
- - Gesloten repositie + onderarmgips op OK3,8
- - Bij voorkeur in electieve omstandigheden binnen 1 week operatie 2,6,7
- - Indien gips niet werkt → Fixateur externe 2,8,9
- - Indien gesloten repositie niet mogelijk
- - Open repositie met K-draden + ligamentair herstel 2,8,9
- Benadering:
- - Dorsaal (mogelijkheid tot overzicht carpale letsel) 10
- - Volair (herstel van volaire kapsel en release van CTS) 10
- Follow-up:
- - Controle 1 week gipskamer voor gipswissel met X-controle
- - Controle 6 weken voor gis af en X-controle en evt. K-draden uit
- - Controle 3 maanden voor functie en X-controle
Complicaties
- Trauma gerelateerd:
- - Gemiste fractuur
- - Posttraumatische artrose
- - N. medianus disfunctie
- - Verminderde bewegelijkheid en kracht van de pols 2,3,8
- Chirurgische gerelateerd:
- - Wondinfectie
- - Materiaalfalen
- - Non-/ malunion
- Ondanks vroeg herkenning prognose tot volledige terugkeer van polsfunctie matig tot slecht 2,3,8
- Lange termijn:
- Bij resterende instabiliteit of delay in diagnose resteert een salvage procedure bijv.:
- - Proximale rij carpectomie
- - Four corner fusion
- - Polsartrodese


Referenties
- 1. Mayfield JK Mechanism of carpal injuries. Clin Ortop relat Res. 1980;149:45-54
- 2. Herzberg G Acute dorsal trans/scaphoid perilunate dislocation, open reduction and internal fixation. Tech Hand Up Extrem. Surg. 2000;4:2-13
- 3. Stanbury SJ, Elfar JC Perilunate dislocation and perilunate fracture-dislocation. J Hand Surg Am. 2008;33:1424-32
- 4. A AOS Comprehensive Orthopeadic review. Section 6: Trauma Chapter 51: Hand and wrist fractures and dislocation, including carpal instability
- 5. Herzberg G, Comtet JJ, Lindscheid RL et al Perilunate dislocations and fracture-dislocations: a multicenter study. J Hand Srug Am. 1993;18:768-79
- 6. Mayfield JK, Kilcoyne RK, Johnson RP. Carpal dislocations: pathomechanics and progressive perilunate instability. J Hand Surg 1980;5:226–241.
- 7. Johnson RPThe acutely injured wrist and its residuals. Clin Orthop 1980;149:33–44.
- 8. Budoff JETreatment of acute lunate and perilunate dislocations. J Hand Surg Am. 2008;33:1424-32
- 9. Blazar PE, Murray P.Treatment of perilunate dislocation by combined dorsal and palmar approaches. Tech Hand Up Extrem Surg. 2001;5:2-7
- 10. Slutsky D, Osterman L. Perilunate injuries of the wrist. In: Slutsky D. Osterman L eds. Fractures and injuries of distal radius and the carpus. Philadephia: Saunders, 2009 Chapter 43