Poplitea aneurysma
Poplitea aneurysma
Auteur: J. Sprakel, MD - Laatste update: 30-10-2019
Poplitea aneurysma
Epidemiologie
- - Arteria Poplitea Aneurysma (APA)
- - Definitie: Progressieve arteriele dilatatie in absolute diameter van a. poplitea (20mm) of 50% vergroting vergeleken met contralaterale a. poplitea 1
- - Incidentie: 0,1-2,8% in algemene bevolking 2-4
- - 5-10% met een APA hebben een AAA 5-7
- - Vooral mannen > 60 jaar
- - Man : vrouw ratio 20:1
- - Oorzaak: Atherosclerose
- Risicofactoren
- - Roken
- - Familiegeschiedenis van hart- of vaatziekte
- - Diabetes mellitus
- - Eerdere hart- en of vaatziekten
- - Hypertensie
- - Hypercholesterolemie
Klinisch beeld
- Asymptomatisch (41%) 8
- Symptomatisch (59%) 8:
- - Acute ischemie * (28%)
- - Chronische ischemie * (21%)
- - Mechanisch (8%)
- - Ruptuur (2%)
- * Perifere ischemie: Claudicatio intermittens, rustpijn of weefselverlies geassocieerd met trombose of embolieen
- Symptomen:
- - Bewustwording van popliteale massa
- - Lokale pijn
- - Zwelling van been door v. poplitea compressie
- - Aanwezigheid APA contralaterale zijde
Anatomie
- Normaal verloop: De a. poplitea loopt door de fossa poplitea en splitst in de a. tibialis anterior (ATA) en de truncus tibiofibularis. Vanuit de truncus splitst deze in de a. tibialis posterior en de a. peronea (fibularis / PR)
- Lengte: 12-18cm
- Normale diameter: 5-9mm
- Poplitea is opgedeeld in 3 segmenten:
- - P1: Tussen de adductor hiatus en de top van de patella
- - P2: Tussen de top van de patella en de knie articulatie
- - P3: Tussen de knie articulatie en de aftakkingen van de crurale arterien
Classificatie
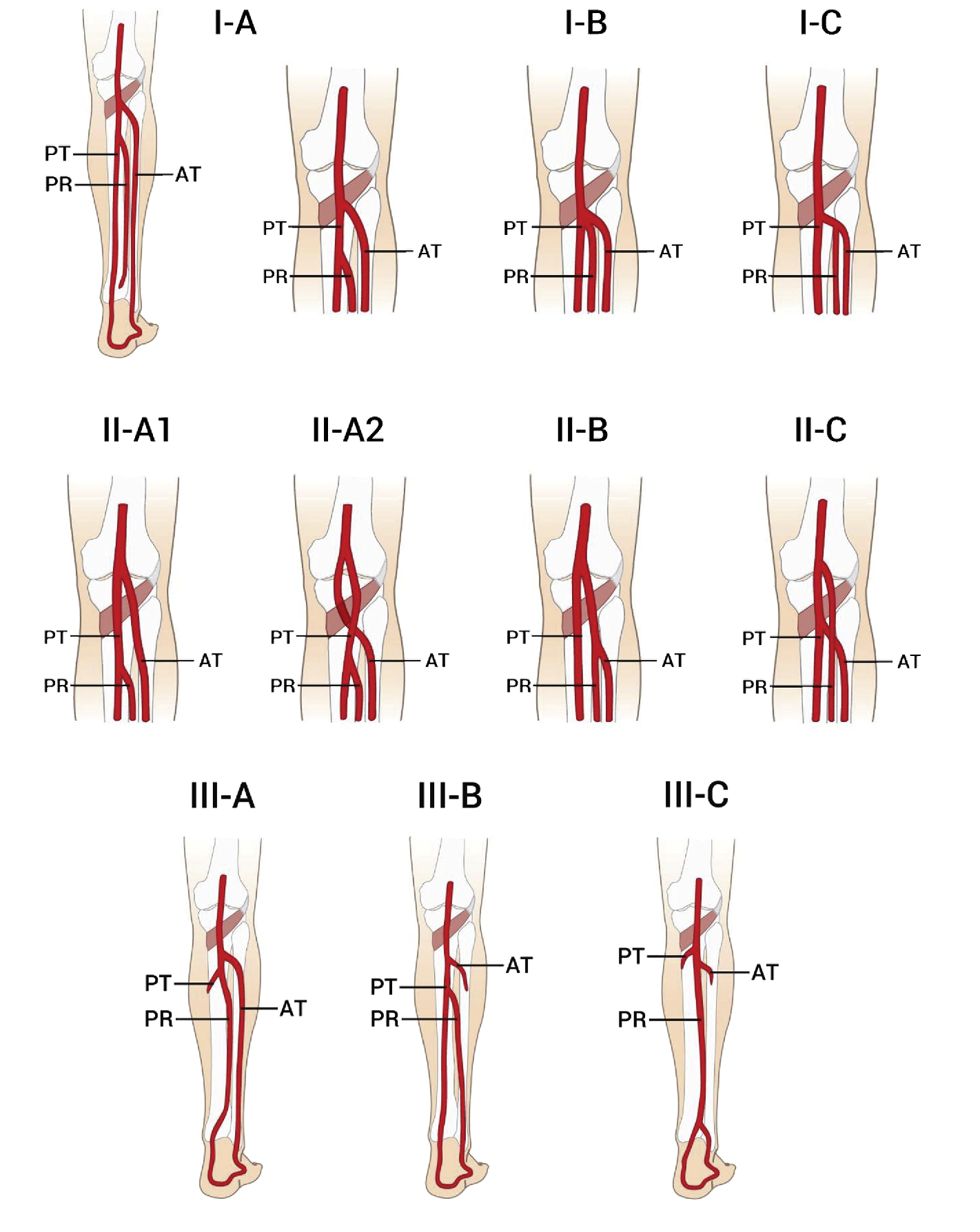
- Classificatie volgen Kim - variaties in vertakking van a. poplitea (9%) 8
- Type 1: Normaal niveau van a. poplitea vertakking
- - IA (91%): Normaal verloop
- - IB (2,4%): Trifurcatie van ATA, PR en ATP binnen 0,5cm, geen echte truncus tibiofibularis
- - IC (1,1%): Splitst in ATP en truncus tibioperonealis
- Type 2: Hoge splitsing van a. poplitea
- - IIA1 (2,2%): Origo van de ATA op niveau of boven het kniegewricht
- - IIA2 (0,3%): Origo van de ATA op niveau of boven het kniegewricht met mediale bocht in de ATA
- - IIB (1,2%): Origo van de ATP op niveau of boven het kniegewricht en truncus tibioperonealis
- - IIC (0,2%): Origo van de PR op niveau of boven het kniegewricht en truncus van ATA en ATP
- Type 3: Hypoplastische of aplastische tak
- - IIIA (1,7%): Hypoplastische of aplastische ATP, distale ATP vervangt door PR
- - IIIB (1,2%): Hypoplastische of aplastische ATP en ATA, a. dorsalis pedis (ADP) vervangt door PR
- - IIIC (0,1%): Hypoplastische of aplastische ATP en ATA, ADP en ATA vervangt door PR
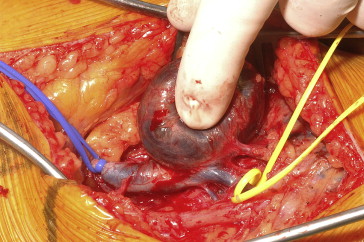
Operatieve behandeling
- Indicatie:
- - Asymptomatisch poplitea aneurysma >30mm
- - Asymptomatisch poplitea aneurysma >20mm met murale trombose
- - Symptomatische poplitea aneurysma van elke grootte (ter voorkoming van distale embolisatie of thrombose)
- Behandeling:
- - Posterieure benadering met autoloog veneus interponaat of polytetrafluroethyleen (PTFE) interponaat
- - Mediale benadering met proximale en distale aneurysma ligatie gevolgd door autoloog veneuze bypass of polytetrafluroethyleen (PTFE)
- - Endovasculaire stent via antegrade punctie in AFC met self-expanding polytetrafluoroethylene nitinol-supported stent (bijv. GORE® VIABAHN® Endoprosthesis)
Complicaties
| 30-dagen complicaties 8: | Open | Endo |
| - Mortaliteit (allen niet gerelateerd aan ingreep): | 2,0% | 1,3% |
| - Amputatie: | 3,2% | 0,0% |
| - Occlusie: | 3,9% | 3,6% |
| - Wond infectie: | 4,7% | 0,0% |
| - Voetheffersparese (klapvoet / n. peroneus): | 1,3% | 0,0% |
| - DVT: | 1,6% | 0,0% |
| - Hematoom: | 3,4% | 0,5% |
| - Endoleak: | X | 4,5% |
- Patencies:
- - Primary patency na 1 jaar: 88,3%
- - Primary patency na 3 jaar: 79.4%
- - Primary patency na 5 jaar: 76% 2-3
- - Secondary patency na 1 jaar: 92.3%
- - Secondary patency na 3 jaar: 86.6%
Referenties
- 1. Davis RP, Neiman HL, Yao JS, Bergan JJ. Ultrasound scan in diagnosis of peripheral aneurysms. Arch Surg. 1977 Jan;112(1):55-8.
- 2. Duffy ST, Colgan MP, Sultan S, Moore DJ, Shanik GD. Popliteal aneurysms: a 10-year experience. Eur J Vasc Endovasc Surg. 1998 Sep;16(3):218-22.
- 3. Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, Halperin JL, Hiratzka LF, Murphy WR, Olin JW, Puschett JB, Rosenfield KA, Sacks D, Stanley JC, Taylor LM Jr, White CJ, White J, White RA, Antman EM, Smith SC Jr, Adams CD, Anderson JL, Faxon DP, Fuster V, Gibbons RJ, Hunt SA, Jacobs AK, Nishimura R, Ornato JP, Page RL, Riegel B; American Association for Vascular Surgery; Society for Vascular Surgery; Society for Cardiovascular Angiography and Interventions; Society for Vascular Medicine and Biology; Society of Interventional Radiology; ACC/AHA Task Force on Practice Guidelines Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease; American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; Vascular Disease Foundation. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation. 2006 Mar 21;113(11):e463-654
- 4. Pulli R, Dorigo W, Troisi N, Innocenti AA, Pratesi G, Azas L, Pratesi C.Surgical management of popliteal artery aneurysms: which factors affect outcomes? J Vasc Surg. 2006 Mar;43(3):481-7.
- 5. MacSweeney ST, Skidmore C, Turner RJ, Sian M, Brown L, Henney AM, Greenhalgh RM, Powell JT.Unravelling the familial tendency to aneurysmal disease: popliteal aneurysm, hypertension and fibrillin genotype. Eur J Vasc Endovasc Surg. 1996 Aug;12(2):162-6.
- 6. Sandgren T, Sonesson B, Ryden-Ahlgren, Länne T.Arterial dimensions in the lower extremities of patients with abdominal aortic aneurysms--no indications of a generalized dilating diathesis. J Vasc Surg. 2001 Dec;34(6):1079-84.
- 7. Diwan A, Sarkar R, Stanley JC, Zelenock GB, Wakefield TW. Incidence of femoral and popliteal artery aneurysms in patients with abdominal aortic aneurysms. J Vasc Surg. 2000 May;31(5):863-9.
- 8. Kropman RH, De Vries JP, Moll FL. Surgical and endovascular treatment of atherosclerotic popliteal artery aneurysms. J Cardiovasc Surg (Torino). 2007 Jun;48(3):281-8.
- 9. Kim D, Orron DE, Skillman JJ.Surgical significance of popliteal arterial variants. A unified angiographic classification. Ann Surg. 1989 Dec;210(6):776-81.
- 10.